Summary
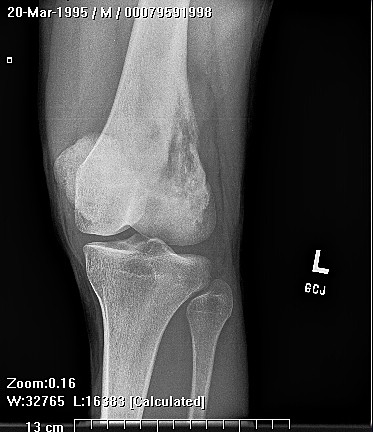
Granulocytic sarcoma (GS) is a solid tumor of immature granulocytes that most commonly occurs in a patient with leukemia or some other myleoproliferative disorder. Osseous lesions are most common in the skull and the orbit.
Complete Information on this Tumor
Granulocytic sarcoma (GS) is a solid tumor of immature granulocytes that most commonly occurs in a patient with leukemia or some other myleoproliferative disorder, but may occasionally occur in an otherwise healthy individual.
The majority of osseous granulocytic sarcomas present with skeletal pain referable to the location of the lesion. This tumor has three characteristic clinical presentations: one, in an individual with no known disease where it is a harbinger of acute myelogenous leukemia; two, in an individual with already known myleoproliferative disorder. Subsequent evaluation of peripheral blood and bone marrow biopsy in this case demonstrated this to be granulocytic sarcoma without systemic evidence of acute myelogenous leukemia. The appearance of the tumor in a previously healthy individual presents a significant diagnostic challenge, and 75% of these cases are usually misdiagnosed.