Summary
Description
Subchondral bone cyst presents as a tumor mimic when a patient with known cancer is found to have a cyst near a joint.
People and Age
This lesion occurs mostly in older individuals, often over 60.
Symptoms and Presentation
This lesion presents with gradual onset of pain in a joint.
Brief description of the xray
This lesion occurs near arthritic joints, especially the hip and knee.
Brief desc of tx
The cyst is treated in the usual manner of treatment for arthritis. Some of these lesions can be eliminated with a minimally invasive procedure.
Tumor Name
Tumor Type
Benign or Malignant
Body region
Location in bone
Periosteal reaction
Position within the bone
Tumor behavior
Case ID Number
Tumor density
Complete Information on this Tumor
Introduction and Definition
In a setting where many older patients or patients with osteoarthritis are seen, osteoarthritic cysts in periarticular bones will be commonly seen . Patients often have pain in the affected joint because of the osteoarthritis, and the radiographs reveal what may seem to be a destructive bone lesion.
Incidence and Demographics
This lesion occurs mostly in older individuals, often over 60, but some patients are in their 40's. Generally found adjacent to a visibly arthritic joint, with joint space narrowing and other radiographic signs of arthritis.
Symptoms and Presentation
Gradual onset and progression of pain in the joint.
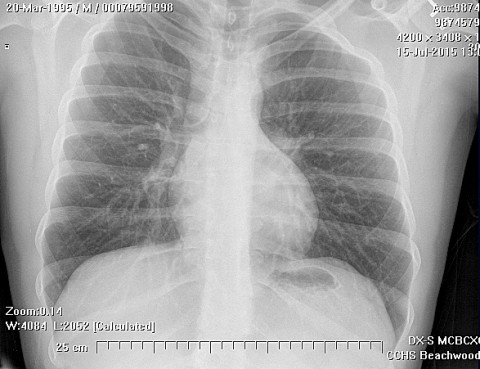
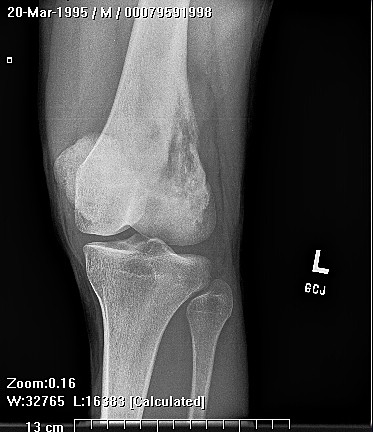
X-Ray Appearance and Advanced Imaging Findings
A lytic, periarticular, weel-defined lesion is seen in a subchondral, marginal, or periarticular position adjacent to the arthritic joint. The lesions usually have a sclerotic rim, and are multilocular. There may be considerable perilesional bone marrow signal change or edema. Careful analysis of the MRI will usually show the connection between the joint and the cyst, which is the channel through which the joint fluid is getting into the bone. The contents of the cyst are bright on T2 and dark on T1 weighted MRI scans.
Differential Diagnosis
To differentiate between these benign entities and a true bone tumor or a metastatic cancer deposit in bone, look for the following features:
1) The lesion is right next to the joint. Careful examination of the radiographs may reveal an actual communication between the joint space and the cyst cavity. If doubt about the nature of the lesion exists, a fine cut CT scan on the area may allow this communicating opening to be seen and help establish the true diagnosis.
2) There are radiographically visible signs of osteoarthritis, usually moderate but sometimes mild, seen in the adjacent joint. If these are entirely absent, the diagnosis should be reconsidered. In the hip, these lesions occur the acetabulum in women with "shallow hips" which can be determined by calculating the center-edge angle. The shallow hip is prone to early degenerative changes and cysts are common in these patients.
3)There is usually a sclerotic rim around some areas of the lesion. The zone of transition is narrow, whereas in a metastatic lesion
4) The lesion should be fluid filled, and this may be seen best on MRI images.
5) These lesions are rarely progressive, and pathological fractures are rare.
1) The lesion is right next to the joint. Careful examination of the radiographs may reveal an actual communication between the joint space and the cyst cavity. If doubt about the nature of the lesion exists, a fine cut CT scan on the area may allow this communicating opening to be seen and help establish the true diagnosis.
2) There are radiographically visible signs of osteoarthritis, usually moderate but sometimes mild, seen in the adjacent joint. If these are entirely absent, the diagnosis should be reconsidered. In the hip, these lesions occur the acetabulum in women with "shallow hips" which can be determined by calculating the center-edge angle. The shallow hip is prone to early degenerative changes and cysts are common in these patients.
3)There is usually a sclerotic rim around some areas of the lesion. The zone of transition is narrow, whereas in a metastatic lesion
4) The lesion should be fluid filled, and this may be seen best on MRI images.
5) These lesions are rarely progressive, and pathological fractures are rare.
Treatment Options for this Tumor
Treatment should be directed towards the cause, which is the lesion in the nearby joint, usually OA or sometimes a meniscus or ligament tear, or a ttaumatic cartilage defect. In our center, we have been using minimally invasive surgery to treat these lesions when they are symptomatic.
Special and Unusual Features
Subchondral bone cyst presents as a tumor mimic due to the following scenario: A patient with a known cancer develops worsening pain in a joint. Although a plain xray would reveal the true nature of the lesion, in some cases MRI is the first imaging modality used. MRI tends to make these lesions look much more worrisome than they really are. The radiologist has no plain xrasy to refer to, (or fails to seek out the plain radiographs that have been made) and reads the MRI without having the benefit of the xrays. The patient's cancer history weighs heavily on the mind of the radiologist, and tents to skew the reading. The radiologist will err on the side of caution and suggests that the cyst might be due to the cancer. This leads to a cancer workup and referral to an orthopedic tumor specialist.