Summary
Description
Osteochondroma is a benign tumor that occurs in areas of bone and cartilage. Tumors are most often found in the long bones, especially near the knee or shoulder. Lesion can either be sessile or pedunculated.
People and Age
Occurs in people aged under 20, with a male to female ratio of 1.5: 1
Symptoms and Presentation
Clinically presents with pain due to mechanical irritation or as a painless mass.
Brief description of the xray
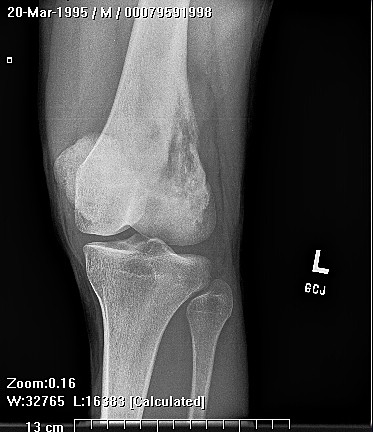
Sessile tumors appears as wide ranging with trumpet-shaped deformity. Pedunculated lesions appear distally.
Complete Information on this Tumor
Introduction and Definition
Osteochondroma, or osteocartilaginous exostosis, is the most common skeletal neoplasm. The cartilage capped subperiosteal bone projection accounts for 20-50% of benign bone tumors and 10-15% of all bone tumors.Osteochondromas are most likely caused by either a congenital defect or trauma of the perichondrium which results in the herniation of a fragment of the epiphyseal growth plate through the periosteal bone cuff. Osteochondromas can either be flattened (sessile) or stalk-like (exostosis) and appear in a juxta-epiphyseal location. Osteochondromas are also the result of radiation therapy in children. After the close of the growth plate in late adolescence there is normally no further growth of the osteochondroma.
Incidence and Demographics
The lesions occur only in bones that develop from cartilage (endochondral ossification). Osteochondromas are found most often in long bones, especially the distal femur and proximal tibia, with 40% of the tumors occurring around the knee.
Osteochondromas occur most frequently in the first two decades of life with a ratio of male to female of 1.5 to 1.
Symptoms and Presentation
Clinically, osteochondromas present with pain due to mechanical irritation or a painless mass. A fracture can occur through the stalk of the lesion which also causes pain.
X-Ray Appearance and Advanced Imaging Findings
Plain films are normally enough to diagnose osteochondromas. Sessile lesions cover a wide area and as a result cause metaphyseal widening or a "trumpet shaped deformity" on x-ray. Lesions with stalks are often found more distally and are common over the posterior femoral metaphysis. CT is helpful in determining if the marrow and cortices of the lesion are continuous with the bone. The relationship of the lesion to other structures and the thickness of the cartilage cap are best delineated
with MRI.
Histopathology findings
On gross examination, an osteochondroma is an irregular bony mass with a bluish gray cap of cartilage. Opaque yellow cartilage has calcification within the matrix. The base of the lesion has a rim of cortical bone and central cancellous bone. Occasionally, a bursae develops over an osteochondroma. Normally, the cartilage cap ranges from 1-6 mm thick. Over 2 cm of cartilage or renewed growth of a dormant lesion are signs of possible malignant transformation.Under the microscope, an osteochondroma has endochondral ossification on the basal surface of hyaline cartilage so it resembles a normal growth plate with rows of chondrocytes. The cartilage is more disorganized than normal, has binucleate chondrocytes in lacunae, and is covered with a thin layer of periosteum.
Treatment Options for this Tumor
There is no treatment necessary for asymptomatic osteochondromas. If the lesion is causing pain or neurologic symptoms due to compression it should be excised at the base.
Outcomes of Treatment and Prognosis
As long as the entire cartilage cap is removed there should be no recurrence. Patients with many especially large osteochondromas should have regular screening exams and radiographs to detect malignant transformation early.
Special and Unusual Features
Hereditary multiple osteochondromatosis is an autosomal dominant condition that can lead to both sessile and pedunculated lesions. The lesions may occur on different bones or on the same bone, and symptoms present in the first decade of life. The risk of malignant transformation to chondrosarcoma in hereditary multiple osteochondromatosis is unknown, but may be 25-30% compared to approximately 1% for a solitary osteochondromas.3 The risk of malignant degeneration increases as the number and size of the osteochondromas increases. In general, a sessile lesion is more likely to degenerate into sarcoma than an exostosis.
Suggested Reading and Reference
References
Giudici, M.A. et al, Cartilaginous Bone Tumors, Radiologic Clinics of North America,31(2):237-259, March 1993.
Bullough, Peter, Orthopaedic Pathology (third edition), Times Mirror International Publishers T Limited, London,1997
Gitelis, S. et al, Benign Bone Tumors, Instructional Course Lectures, 45:42646, 1991.
Huvos, Andrew, Bone Tumors: Diagnosis. Treatment and Prognosis, W.B. Saunders, Co., 1991.